Why should the collective pay for transition surgery, and does that argument hold?
Three questions that are constantly taken for one, and what each one can really answer
0. Introduction: one question, taken for one, that is really three
Few health expenditures trigger a “why should I pay for this” as immediate as transition surgery. The question touches on public money, on opposed moral convictions and on a reality that many know poorly, and this accumulation explains why the confusion between “is it effective”, “is it affordable” and “is it my role to fund this” is at its most frequent and its most heated here. The debate flares up all the faster because it mixes registers that do not obey the same rules.
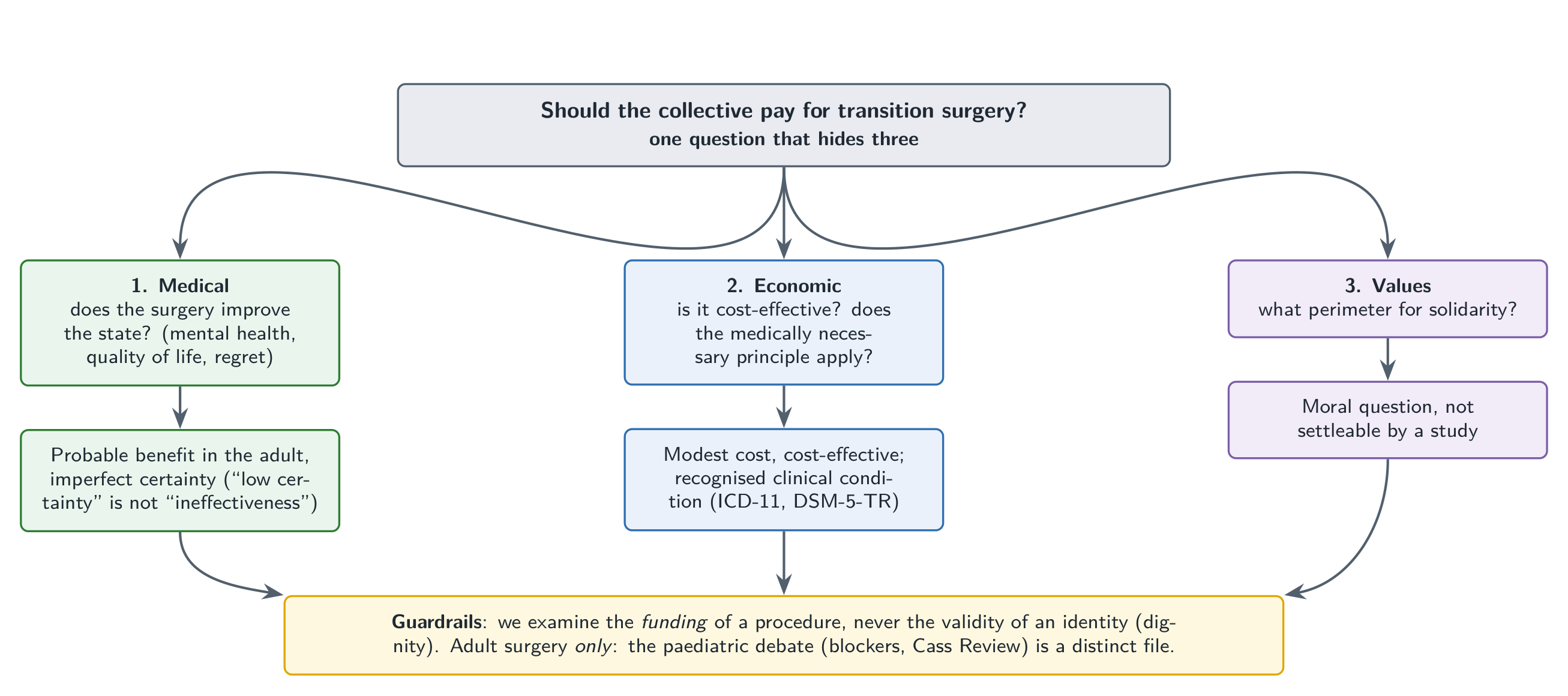
That is the starting point of this text. “Should the collective pay for sex-reassignment surgery?” presents itself as a single question, when it contains three, nested, which public debate constantly conflates: a medical question (does the surgery really improve the state of the people operated on, their mental health, their quality of life, and at what rate of regret?), an economic and insurance question (is the care cost-effective, and does the principle of “medically necessary” apply to it?), and a question of values (how far should the perimeter of solidarity extend, and who decides its boundary?). Each calls for a different kind of answer, and mixing them produces dialogues of the deaf where one believes one is debating the same object. The medical question awaits data; the economic question awaits orders of magnitude; the question of values awaits a collective deliberation, and none of them is settled with the tools of another. The thesis defended here is modest in its form and demanding in its method: the funding argument is solid when one keeps these three questions separate and sticks to adult surgery, and it falls apart as soon as one mixes them or makes it carry another file.
The approach of this paper consists in examining under what conditions the funding argument holds, keeping the three questions separate and limiting itself to the surgery of the consenting adult. The aim is not to tell anyone how to vote; it is to return each question to its proper level, so that one knows, at every moment of the debate, which of the three one is dealing with.
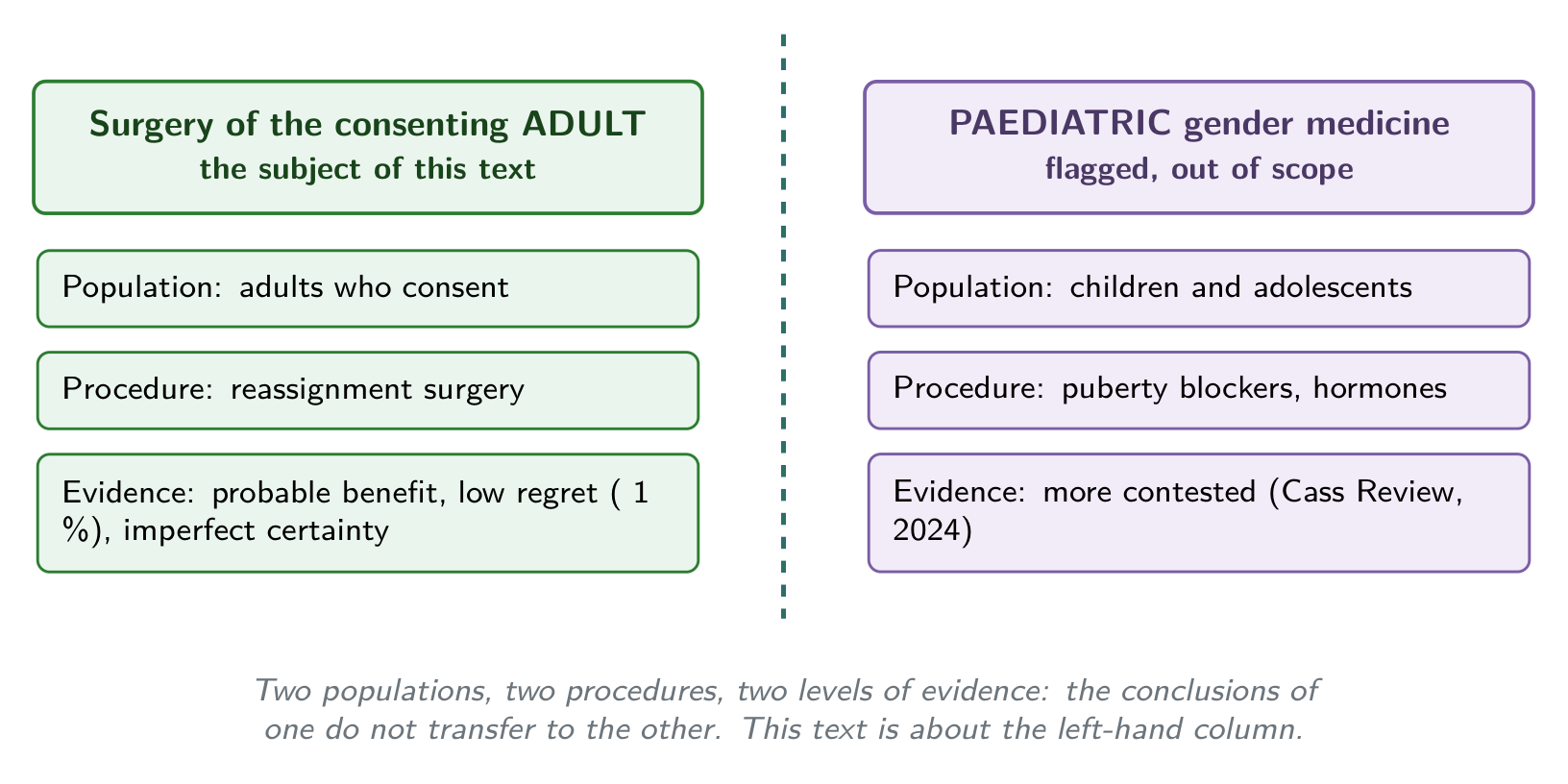
Two guardrails frame everything that follows, and they are not negotiable. The first concerns dignity: this text is about the funding of a medical procedure, never about the validity of an identity, and it never treats being transgender as a delusion, a fashion or an illness to be cured. The second concerns the precision of the scope: the object is the collective funding of reassignment surgery in the consenting adult, whereas paediatric gender medicine and puberty blockers form a distinct file, with another population, another procedure and another level of evidence, flagged here without being the subject. Conflating these two files is one of the most common sources of error in the debate, and avoiding it is a condition of rigour, not a convenience.
1. What are we talking about: laying out the object cleanly
Before asking whether a form of care deserves to be funded, one must specify which care and which condition one is talking about, without which the debate floats. Gender dysphoria, or gender incongruence, is a clinical condition recognised by the reference nosographies, and this point is not an administrative detail: it conditions the very entry into insurance logic. The World Health Organization’s International Classification of Diseases, in its eleventh revision, recognises gender incongruence and has explicitly removed it from the chapter on mental disorders to classify it among conditions related to sexual health (Organisation mondiale de la Santé 2019; Reed et al. 2016). This shift depathologises the identity while maintaining a clinical code that allows access to care, and it illustrates the distinction the whole paper holds: a condition can call for care without being a disorder of the mind. The revision was explicit on this point, separating gender incongruence from mental disorders while keeping it in the classification so as not to deprive the people concerned of a gateway into the care system (Organisation mondiale de la Santé 2019; Reed et al. 2016).
On the North American side, the American Psychiatric Association’s DSM-5-TR recognises gender dysphoria as a clinical diagnosis, defined by a clinically significant distress linked to the incongruence between lived gender and assigned sex (American Psychiatric Association 2022; Reed et al. 2016). The diagnosis therefore bears on the distress and on its impact, not on the fact of being transgender, which answers in advance the false idea that recognising a condition would amount to judging an identity.
Part of this distress does not come from an intrinsic pathology. The minority stress model attributes a fraction of the excess psychic distress of transgender people to stigma, discrimination and rejection, which locates part of the burden on the side of the social environment rather than of an individual defect (Meyer 2003; Bockting et al. 2013). This framework matters for what follows, because it clarifies why care can target the incongruence itself when another part of the suffering stems from social conditions that medicine does not treat.
The procedure, next. Reassignment surgery in the adult falls within a framework of professional standards, foremost among them WPATH’s Standards of Care 8 published in 2022, which set criteria of indication, assessment and consent, and not a procedure granted without condition (Coleman et al. 2022; Hembree et al. 2017). These same standards generally provide for a prior assessment pathway, which distinguishes the funded procedure from an immediate request and answers in part the objection of care “on simple demand” (Coleman et al. 2022). The Endocrine Society’s guidelines frame, for their part, the medical treatment of gender dysphoria in the adult, which situates surgery within a structured care pathway rather than a one-off request (Hembree et al. 2017). We are therefore talking about a signposted procedure, indicated at the end of a process, not an improvised act.
One must also place this procedure in time. Reassignment surgery has been practised and studied for decades, so that the debate on its funding does not bear on a recent experimental technique; it bears on an established medical procedure in the adult (Coleman et al. 2022). Finally, and this point governs the whole reading, reassignment surgery in the consenting adult is a population and a procedure distinct from paediatric gender medicine: the conclusions and the level of evidence of one do not transfer to the other. Every time public debate imports into the adult file an objection born of the paediatric file, it commits a category error that what follows takes care not to reproduce. The population, the procedure, the degree of reversibility and the level of evidence differ from one file to the other, so that an argument valid in one may be without bearing in the other. This section has therefore not only described an object; it has set the bounds within which the three following questions keep a meaning.
2. The medical question: does the surgery improve people’s state?
This is the first of the three questions, and it is a question of facts: it has answers, imperfect ones, that can be given without campaigning. An honest reading of the literature requires holding both ends at once, the real signal and its limits, without over-rating either.
The signal, first. Systematic reviews of quality of life and mental health after reassignment surgery in the adult generally report an improvement, while underlining an evidence base of moderate to low certainty, made up mostly of observational studies, without a control group and with losses to follow-up (Murad et al. 2010; Almazan and Keuroghlian 2021). The result therefore points toward a benefit, and its methodological robustness remains limited, two findings that must be stated together. Several studies also associate access to the desired transition care with a reduction in suicidal ideation and distress, an encouraging result, of limited certainty owing to possible confounds and self-selection, to be cited without making it a definitive demonstration (Almazan and Keuroghlian 2021).
Regret, next, often at the centre of the debate. Meta-analyses of adult cohorts report a rate of regret after reassignment surgery on the order of 1%, low compared with the regret rates of other major medical interventions (“Regret After Gender-Affirmation Surgery” 2022; Wiepjes et al. 2018). This figure must be read with caution in both directions: losses to follow-up, the heterogeneity of definitions of regret and sometimes short follow-ups may underestimate it, which invites one not to over-rate the favourable literature (“Regret After Gender-Affirmation Surgery” 2022). A low rate is still a low rate, and the uncertainty about its exact measure remains.
Regret is not to be confused with detransition, often invoked. Detransition exists and has heterogeneous causes, the evolution of identity as much as social pressures, discrimination or complications, so that it is not read mechanically as a regret of the medical transition (Turban et al. 2021; Wiepjes et al. 2018). Making it a proof of the failure of the care would be a forced reading; ignoring it would be just as dishonest. A person who interrupts or reverses their transition because they suffer family or professional rejection says little about the effect of the medical act on their dysphoria; they say above all something about their environment. Another whose identity has evolved comes closer to a regret in the proper sense, and the two cases are not read the same way (Turban et al. 2021; Wiepjes et al. 2018). Conflating the two amounts to charging to the care what stems from social conditions, exactly the opposite of the caution the subject demands.
The field is fragile, and this must be said without dramatising. A widely cited national cohort study first associated surgery with a decrease in the subsequent use of mental health care, before a reanalysis and a correction published attenuated this result, an illustration to be cited symmetrically of the caution called for (Bränström and Pachankis 2020). In the other direction, a long-term Swedish cohort showed a psychiatric mortality and morbidity higher than that of the general population after reassignment, a result often misquoted: its authors themselves stress that it does not establish the ineffectiveness of surgery and that it does not compare with untreated transgender people (Dhejne et al. 2011). These two examples, taken together, show that neither side has a decisive datum, and that the isolated citation of a study often serves a thesis it does not support. The Swedish cohort is regularly brandished as proof that surgery is useless, whereas its authors warn against this use and recall the absence of a relevant comparison group (Dhejne et al. 2011). The reanalysis of the more favourable cohort, conversely, invites one not to over-invest a single result in the other direction (Bränström and Pachankis 2020). The common lesson is the same: on this subject, a figure taken out of its study almost always lies by omitting its limits.
One must add to the balance what a surgery carries in the way of risk. Like any major surgery, reassignment surgery presents non-negligible rates of complications depending on the techniques, a datum to be integrated honestly into the benefit-risk balance and into the cost models (Jacobs and Ferrando 2025). Passing over these complications in silence would distort the picture as much as denying the benefit. An honest balance records both the probable gain in quality of life and the operative risk proper to each technique, and it is this balance, not an isolated figure, that informs the coverage decision (Jacobs and Ferrando 2025).
Then comes the most important distinction of this section, the one that separates a legitimate skepticism from an unfair trial. The reference systematic reviews often conclude to a “low” certainty of the evidence, which means an uncertainty about the magnitude of the effect, and not a proof of ineffectiveness: the two must never be confused. Evidence of low certainty calls for caution about the size of the benefit; it does not authorise concluding to the absence of benefit. It is precisely on this point that a file is regularly transferred wrongly. The Cass Review, published in 2024 and often invoked for its conclusion of low certainty, bears on the gender medicine of children and adolescents, a population and procedures distinct from adult surgery, and cannot therefore be transposed as such to the latter (Cass 2024; Taylor et al. 2024). Importing its conclusions into the adult file is to conflate two questions that everything separates.
There remains a requirement of symmetry about the standard of evidence itself. The fact that the evidence base is imperfect is real, and it is shared by many established surgical fields, where the randomised trial is difficult or even impossible for ethical and practical reasons; demanding here a level of evidence one does not demand elsewhere would be an asymmetric criterion. The distinction between low certainty and ineffectiveness deserves to be repeated, so trampled is it in the debate. A review that notes “low certainty” describes the state of the literature, the scarcity of controlled trials and the presence of biases, and it pronounces no verdict on the existence of the benefit; reading one for the other inverts the meaning of the conclusion. Symmetrically, methodological caution must not turn into an impossible demand: to claim for this care the double-blind randomised trial that one demands of no comparable surgery would amount to setting a bar that surgical medicine almost never clears. The calibrated conclusion of this section therefore holds in one sentence: in the operated adult, the benefit is probable and the evidence imperfect, which is neither a certainty nor a refutation.
3. The economic question: is it cost-effective?
Second question of facts, distinct from the previous one: assuming a benefit, is the care a reasonable use of resources? The answer runs through orders of magnitude, to be handled with the same caution as the medical data they inherit.
On cost-utility, analyses estimate that the coverage of transition, surgery included, falls within a range of cost per quality-adjusted life year, the QALY, comparable to that of other commonly reimbursed care (Padula et al. 2016). In other words, related to the benefit it aims at, the care does not appear as an aberrant expenditure with regard to the thresholds that systems already apply. These analyses rest, however, on uncertain assumptions, the magnitude of the benefit, its duration, the rate of complications, inherited from the limited certainty of evidence of the previous section, and they must therefore be read as orders of magnitude, not as verdicts. Intellectual coherence requires it: one cannot invoke medical uncertainty to doubt the benefit, then treat the economic models that depend on it as certainties.
On the budgetary weight, next. The item that the funding of reassignment surgery would represent is modest with regard to the whole of health expenditure, which limits the reach of the pure budgetary argument (Padula et al. 2016). This finding holds by two factors that combine: an ordinary unit cost and a restricted population concerned. The unit cost of a reassignment surgery falls within the order of magnitude of other commonly covered surgical interventions, which deprives the “exorbitant cost” argument of empirical foundation (Padula et al. 2016). And the proportion of people concerned by a request for surgery remains low in the population, which bounds the budgetary stake and distinguishes the question of principle, should one cover, from its real magnitude (Meerwijk and Sevelius 2017). One must add a point of method that holds for this whole section. Cost-utility analyses are not direct measures; they are models that aggregate an estimated benefit, an assumed duration and an anticipated risk, and their result is worth what these inputs are worth, themselves marked by the medical uncertainty already flagged. Presenting them as quantified verdicts would give a false impression of precision; presenting them as order-of-magnitude benchmarks is the honest reading (Padula et al. 2016). The question “should one fund” is therefore not settled by the amount, because the amount is small; it shifts elsewhere, toward the principle and toward the values.
4. The insurance principle: what does solidarity already fund?
Here the pivot between facts and values is at play, and it is often the link the debate skips. The operative criterion of solidarity-based health systems is not “what everyone approves of”; it is “the medically necessary for a recognised condition”, which shifts the question from moral taste to clinical indication. Retaining “the medically necessary” as arbiter of the perimeter is itself, moreover, an assumed choice of values, symmetric to the one this text concedes for the boundary of solidarity, and not a neutral theorem. This shift changes everything, for it takes from the individual moral vote the power to decide item by item what the collective reimburses.
Now the procedure in question enters this criterion according to the bodies that define it. Learned societies and health authorities qualify certain reassignment surgeries as medically necessary to treat gender dysphoria in the adult, which brings them into the usual insurance criterion (Coleman et al. 2022; American Medical Association et associations médicales 2021). Large medical associations likewise consider the coverage of transition care, surgery included for the retained indications, as belonging to care founded on the available evidence, a position that weighs in the definition of the medically necessary (American Medical Association et associations médicales 2021; Coleman et al. 2022). These positions do not close the question of values; they answer the question of fact “does this procedure belong to care”, in the affirmative under conditions.
The collective funding of this procedure is, moreover, not a hypothesis: it is a reality already framed. In Switzerland, compulsory health insurance, the LAMal, covers services linked to transition under conditions of indication, which shows that this funding already exists within a regulated framework (Confédération suisse 2023; Padula et al. 2016). More broadly, several public systems and large insurers cover reassignment surgery under conditions, for example in the United States, where the Medicare exclusion dating from 1981 was invalidated in 2014, subsequently opening a case-by-case coverage, as well as various European countries, which situates this procedure within a widespread practice and not in a singularity (Centers for Medicare and Medicaid Services 2014; Padula et al. 2016). The debate therefore does not bear on the opening of an unprecedented right; it bears on the legitimacy of an existing practice.
There remains the coherence argument, which is the heart of this section. Solidarity-based systems already fund care that some taxpayers disapprove of or judge linked to life choices, for example certain coverage of procreation, of addictions or of injuries linked to risk activities, so that objecting to the funding of transition alone requires a criterion that does not, in passing, disqualify part of what one covers without debate. In other words, the criterion “I morally disapprove, so we do not reimburse” would prove too much, for it would also undo a broad part of what everyone finds normal to cover. The criterion of the medically necessary is not suspended by the fact that part of the public disapproves of the procedure; otherwise, the coverage of many forms of care would depend on a majority moral vote, which the insurance principle precisely excludes.
One last point links the insurance to the economic. Refusing the reimbursement of an effective care for a recognised condition can shift the cost elsewhere, toward mental health care, the loss of activity or the complications of unregulated procedures, so that non-funding is not necessarily a net saving. This argument is formulated with caution, backed by the imperfect QALYs of the previous section, and it does not claim to settle anything; it only recalls that an avoided expenditure is not always an expenditure spared. One may summarise the contribution of this section thus: solidarity does not reimburse what pleases, it reimburses what treats a recognised condition, and by this measure the procedure belongs to the usual criterion rather than to an exceptional favour. The fact that other systems already cover it, and that Switzerland does so under conditions, takes from the objection its air of exception: the debate bears on the maintenance of a practice, not on the opening of a breach (Confédération suisse 2023; Padula et al. 2016).
5. The objection of values, in its strongest form
An honest examination does not caricature what it contests; it lays it out in its most solid version before answering it. The objection of values, in its strongest form, breaks down into three: the refusal to fund a procedure one morally disapproves of, in the name of the taxpayer’s freedom of conscience; the doubt about the medical necessity of the care; and prioritisation under limited resources. These three objections are real, and it would be dishonest to treat them as mere prejudices.
They must still be sorted by level, for they do not belong to the same register. The objection “questionable medical necessity” belongs to facts and is treated by evidence, that of the previous sections, a recognised condition and a probable benefit in the adult with imperfect certainty; whereas “I do not want to fund what I disapprove of” and “it is not the priority” belong to arbitrations of values, not settleable by a study. This sorting is decisive, for it shows that only one of the three objections is settled by the data, and that the other two belong to a debate that facts do not arbitrate.
Taking these two objections of values seriously also means measuring their real reach. The taxpayer’s freedom of conscience, taken seriously, cannot ground an individual right of veto over every item of public expenditure without rendering any solidarity-based system unworkable, which does not annul the objection; it shows its limit. Everyone funds through tax expenditures they disapprove of, and it is the very condition of a solidarity that does not dissolve at the first disagreement. Likewise, the argument of prioritisation under limited resources is real, and it is general: it holds against any item of expenditure, and it targets transition only at the price of a choice, itself of values, about what deserves to be funded first. Invoking priorities therefore does not single out transition in particular; it refers to a hierarchy of values that must be assumed as such. Recognising the force of these objections is not yielding to them; it is situating them, and a well-situated objection is discussed better than a caricatured objection. Sorting by level moreover makes the debate more courteous: the one who doubts the effectiveness and the one who refuses out of conviction do not defend the same thing, and conflating them feeds a reciprocal trial of intent that clarity dissolves.
6. The core: not confusing the three questions
Everything that precedes converges toward a single point of method, and it is here that it is formulated. Showing that an objection to funding is of a moral order does not disqualify it; showing that a care is effective does not suffice either to close the funding question: the origin of a position does not decide its value, and a question of values is not closed by a datum. This double prohibition protects both camps at once, for it prevents as much the disqualifying of a moral unease by calling it “only moral” as the closing of a societal disagreement by brandishing a study.
The most common flaw of the debate has a name. The motte-and-bailey consists in contesting effectiveness, a question of facts, so as in reality to carry an objection of values, or in invoking values to settle a question of facts; each camp gains by knowing which of the three questions it is really posing. One believes one is debating the benefit when one is debating the perimeter of solidarity, or the reverse, and the disagreement becomes insoluble for lack of being posed at the right level.
The test of symmetry, here, deserves a clarification that avoids a frequent misreading. It does not “undo” the question: since the factual premise, is the care necessary and effective, can really differ from one procedure to another, symmetry refers to the examination of facts, whereas the disagreement of values about the perimeter remains, for its part, to be assumed. In other words, comparing transition to another care is legitimate only if one also compares the facts, and it never dissolves the properly political part of the disagreement.
This framing has, finally, a requirement of dignity. Clearly distinguishing the question of funding from that of the validity of transgender identities is also a requirement of rigour: conflating them would pass a judgment of identity for a budgetary argument, and conversely, which this paper refuses. Separating the registers is not a precaution of language; it is the condition for each argument to be judged on its own ground. The same principle protects the person concerned: because the paper discusses the funding of a procedure, it does not have to pronounce on the legitimacy of an identity, and it refuses that one serve as a masked argument for the other. This is also what makes the examination sustainable on both sides: the one who approves of the funding and the one who contests it can agree on the map of questions before diverging on the answer, and that disagreement, posed at the right level, remains a disagreement between citizens rather than a clash of camps.
7. Where the argument holds, where the disagreement is legitimate
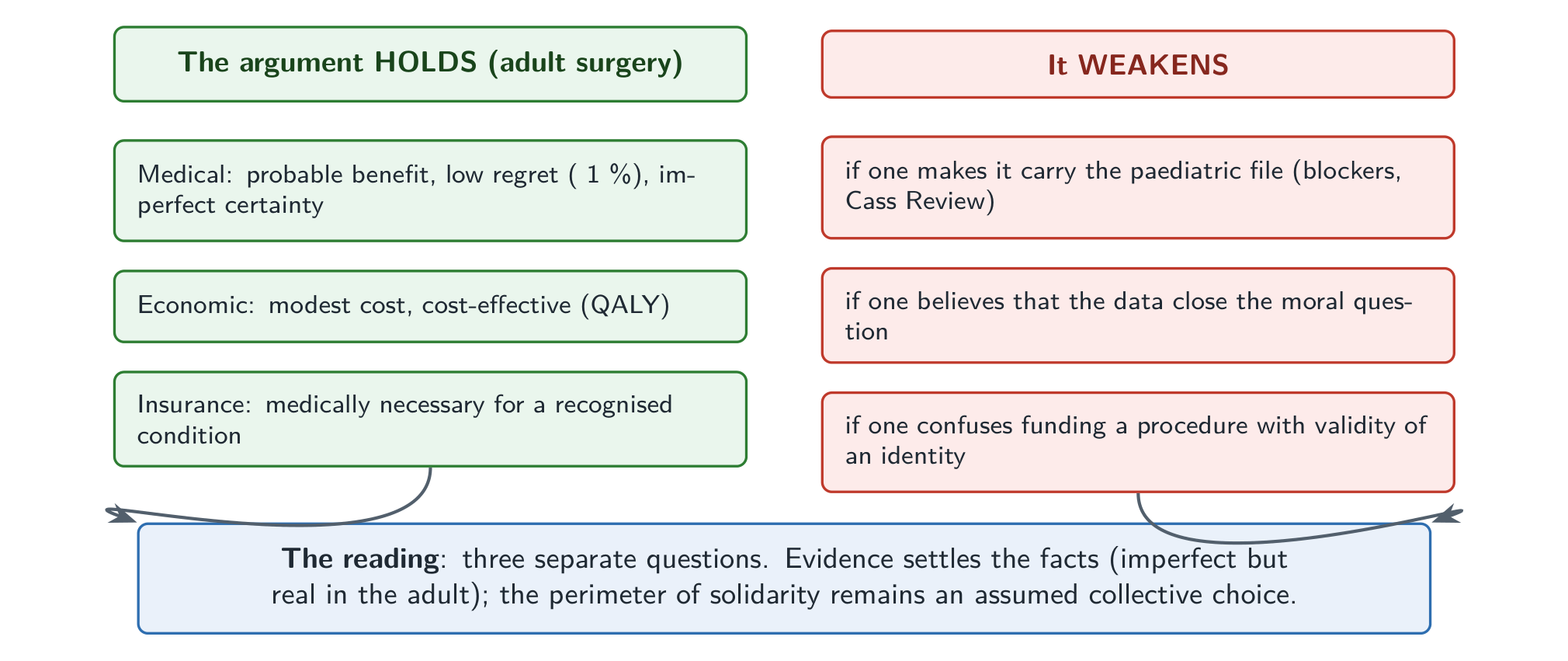
One can now draw up the assessment, without campaigning, returning to each question its answer. The funding argument holds for adult surgery on all three planes: a probable benefit with imperfect certainty on the medical plane, a modest cost compatible with the usual thresholds on the economic plane, and an entry into the criterion of the medically necessary for a recognised condition on the insurance plane. On the sole plane of coherence, the burden of proof weighs rather on whoever would single out this procedure among other already covered forms of care; the perimeter of solidarity, for its part, remains an open choice, with no presumption of a losing camp.
The argument weakens, by contrast, in two precise cases. It weakens if one makes it carry the paediatric file, where the evidence is more contested and the population different, or if one believes that the data close the moral question of the perimeter of solidarity: that is where the legitimate disagreement lodges. The first case is an error of fact, the confusion of two files; the second is the reminder that a question of values stays open even when the facts are established. One can adhere without reserve to the data on adult surgery and continue to debate the perimeter that solidarity must cover, for this perimeter is a choice, not a theorem. Conversely, one can find the societal choice obvious and get the wrong file by lending it the uncertainties of the paediatric side, which do not concern it.
This legitimate disagreement nonetheless leaves room for common ground. The possible point of agreement between opposed camps is methodological: recognising that the medical question has imperfect but benefit-oriented answers in the adult, and that the question of the perimeter of solidarity remains a legitimate collective choice, without disguising one as the other. One can diverge on the final choice while agreeing on the map of questions, and that is already a considerable progress on the usual debate.
The proposed reading remains, finally, falsifiable, as any honest thesis must be. The thesis “the funding argument holds for adult surgery” would be weakened by robust systematic reviews showing the absence of benefit or a high regret in the adult, or by a solid unfavourable cost-utility analysis. It therefore does not protect itself from refutation; it indicates what would overturn it, and it is on this condition that it deserves to be followed.
8. Conclusion: shifting the reading
The whole point lies in a shift of reading. Moving from “should one pay for this” taken as an indistinct block to three distinct questions, what does the medical evidence say, what does the economics say, what perimeter of solidarity does one choose, allows one to answer the questions of fact without campaigning and to leave open, as is fitting, the question of values. The first reading condemns one to the dialogue of the deaf; the second returns to each the part of the question that belongs to them.
The assessment then boils down to a tenable instruction. Treat the medical question with the evidence, imperfect but real in the adult, the economic question with the orders of magnitude, a modest cost, and the question of the perimeter as an assumed choice of values, refusing any slide from one register to another. The facts have answers that one can give without taking sides; the societal choice, for its part, remains to be made, and there is nothing abnormal in its remaining discussed. Separating the three questions tells no one what to decide; it only makes the debate possible on what, in “should one pay for this”, can be established, and on what must remain a choice.